Six months into the worst Ebola epidemic in history, the world is losing the battle to contain it"
Joanne Liu, president of Doctors without Borders at the UN Special Briefing on 2 September 2014
Since January 2014, an Ebola epidemic has been spreading through West Africa, affecting mainly Guinea, Sierra Leone and Liberia, causing several thousand deaths in these countries. While on the one hand the spreading of this virus is cause for worry among the international community as a result of a few Americans and Europeans having been diagnosed as suffering from Ebola virus disease (EVD), on the other hand good news seems to be coming from the African front, especially in Nigeria and DRC where EVD outbreak has been declared over after it has played havoc in these countries during several months. This extremely serious hemorrhagic fever, which first appeared in Sudan and Zaire (now DRC) in 1976, often proves fatal in humans.
1. What is Ebola ?
Ebola virus disease belongs to the Filoviridae family. “Filo” because it resembles a microscopic filament. The Ebola virus is one of the most deadly diseases on the planet. It ranks level 4 in the classification of infectious biological agents.

The Ebola virus comes in 5 strains :
Zaire ebola virus
Sudan ebola virus
Bundibugyo ebola virus
Reston ebola virus
Taï Forest virus
The first three are associated with human epidemics. The Zaire strain is responsible for the outbreak currently affecting West Africa.
The Reston and Taï Forest strains are not associated with major human epidemics, and no deaths have been reported to date. The Reston strain has been identified in the Philippines and in the People’s Republic of China, where it mainly affects monkeys and pigs.
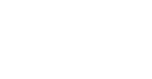
THE ORIGIN OF THE 2014 EPIDEMIC
Although the origin of the virus is still unknown, fruit bats are considered to be the natural reservoir. The main carriers most likely to transmit the disease are gorillas, chimpanzees and antelopes. Contamination passes from animals to humans either through handling the flesh of these infected animals, or eating them, particularly if insufficiently cooked.
 Two theories currently attempt to explain the origin of the 2014 epidemic :
Two theories currently attempt to explain the origin of the 2014 epidemic :
1- According to a team of British researchers,
a two-year-old Guinean child may be at the root of the epidemic.
2- Another study published in the journal Science attributes the start of the epidemic to a faith healer living in Sokoma, Sierra Leone close to the Guinean border.
2. Why does Ebola spread so fast?
This is the first time that the Ebola virus has struck urban zones. Population density fosters transmission and could be the main reason for the current rapid spread of the disease. Contrary to popular belief, recent mutations in the virus do not seem to be the cause. However, these mutations have modified the virus’s pathogenic nature. The death rate was 90% in 1976, compared to 50% to 70% now.
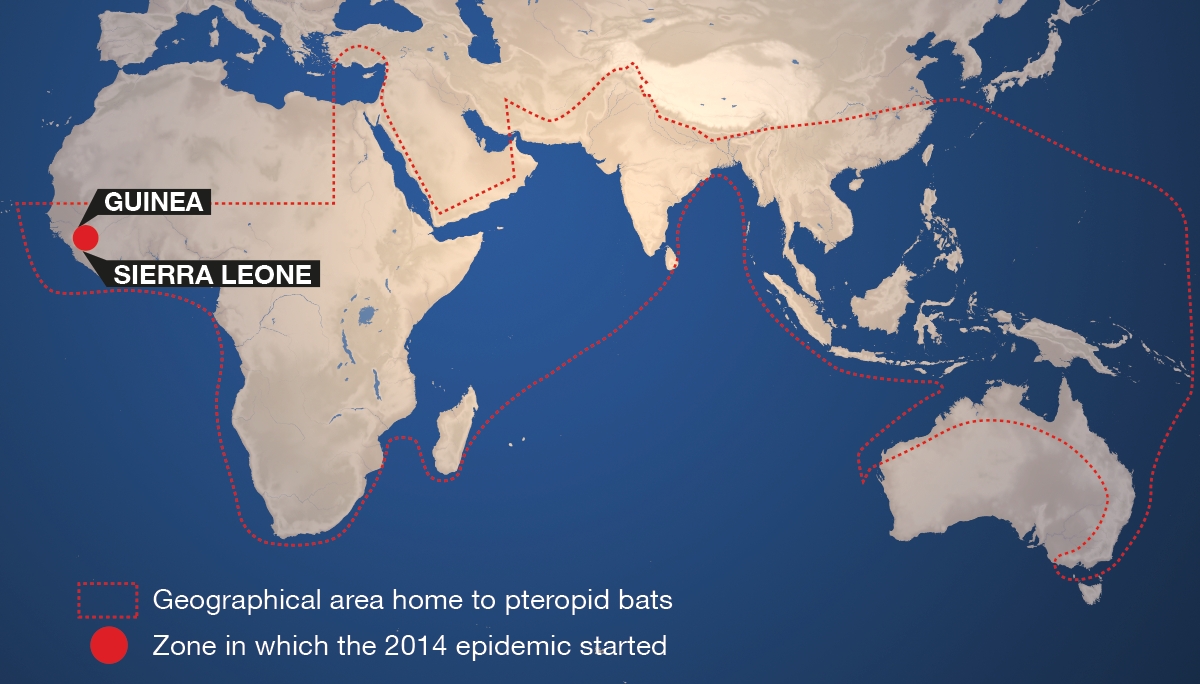
Ebola virus disease invades the infected person’s blood and cells. As the disease progresses, it generally attacks the vital organs, especially the kidneys and liver, and causes significant internal bleeding. Death can occur a short time after the first symptoms, caused by the failure of numerous organs and cardio-respiratory arrest.
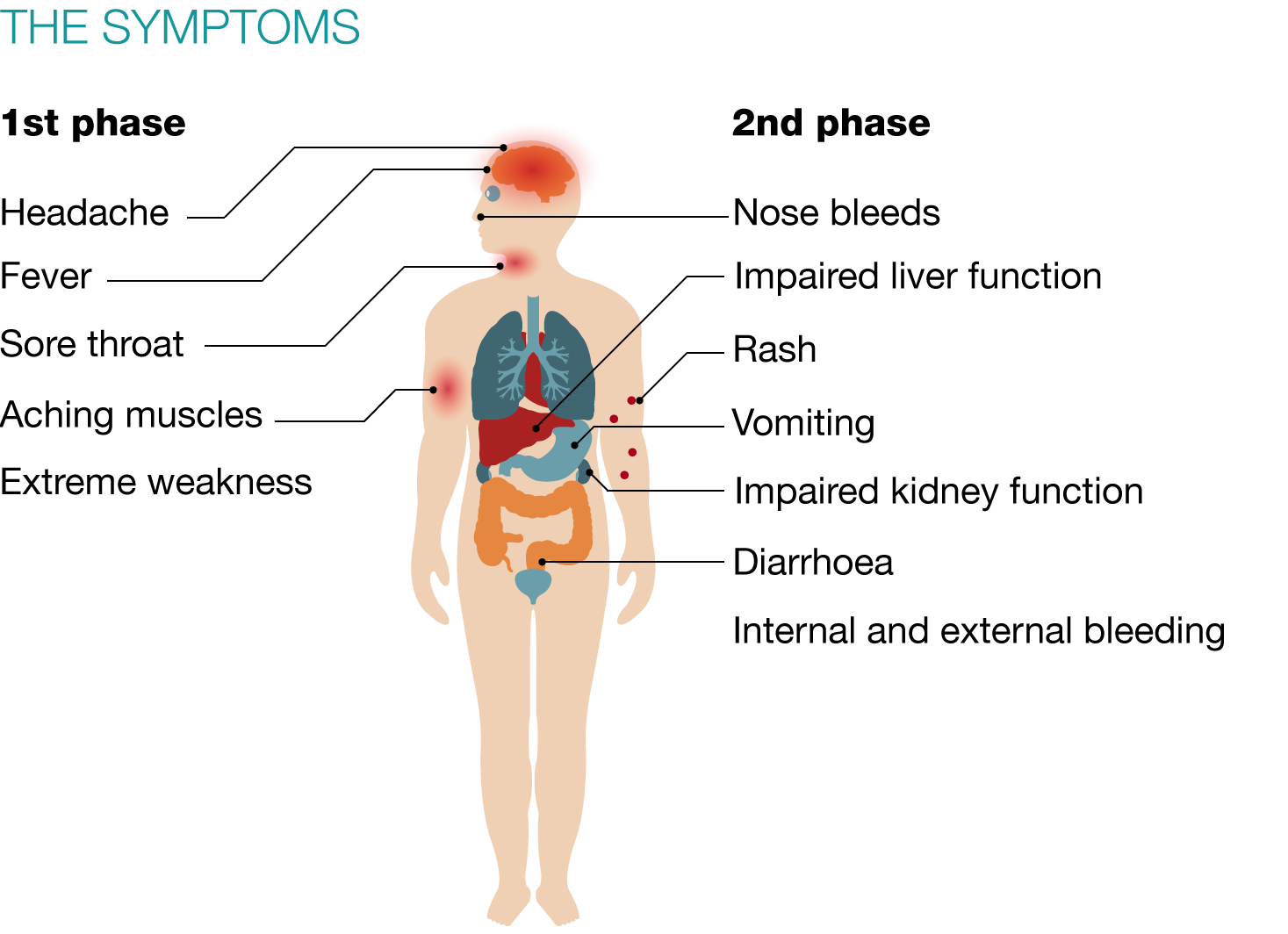
HOW THE DISEASE EVOLVES :
Transmission between humans occurs from contact with the blood, secretions (sneezing) or biological liquids (saliva, blood, urine, faeces, vomit, sperm, sweat) of an infected person or via a contaminated environment.
<
3. What are the ways to avoid contamination?
- Avoid all bodily contact (embraces, handshakes, etc.)
- Wash hands as frequently as possible with soap and water
- Do not sleep in the same room as an Ebola patient
- Do not remain close to an Ebola patient without protection
- Do not touch clothes and other objects soiled by sufferers
- Avoid all contact with vomit, blood or faeces from a person who is suffering or has suffered from Ebola
- Anyone showing symptoms of the disease must immediately contact the nearest health centre
- Care workers should be protected by personal protective equipment (PPE)
- Patients’ clothes and sheets should be handled and burned by specialists wearing personal protective equipment
- Do not touch and/or wash corpses, which should be buried by care workers
- Receive injections in protective conditions in line with standards
- Avoid practising traditional scarring and tattooing during the epidemic
- Do not touch or eat any animals found dead in the forest
- Following recovery: sexual relations with a condom during 3 months, or no sexual relations for 3 months (the virus remains active in sperm during this time).
(Sources CDC, WHO, MSF)

<
4. How are sufferers cared for?
A patient displaying symptoms of the disease at a health centre is placed in isolation. Once a diagnosis has been established, he or she receives treatment for secondary infections. Care workers attempt to find anyone with whom the sufferer has been in physical contact. All those who have touched him or her are then put in observation quarantine for 21 days and their temperature is checked daily. Once the observation period is over, in the absence of a fever, these people are considered as not infected.
WHO has stated that, "people who receive treatment fast can recover". In health centres, patients can receive care and support treatment throughout the course of the disease.
WHAT DOES AN EBOLA TREATMENT CENTRE LOOK LIKE ?
Move your mouse over the image to see the captions :
<
5. Why has WHO authorised the use of test-phase treatments?
To date, no vaccine or certified medication exists to combat the Ebola virus disease.
Patients receive intensive care to treat the symptoms and secondary infections. Most are dehydrated and are either put on a drip or receive oral rehydration solutions.

Up till now, pharmaceutical laboratories had shown little interest in researching the Ebola virus because the disease was restricted to poor countries and had only infected a small number of people. However, the impressive progression of the 2014 epidemic has spurred international research and the World Health Organization has given experimental treatments the go-ahead.
WHO’s ethics experts have authorised clinical trials of unapproved treatments on certain conditions :
- total transparency of type of treatment
- freedom of choice and guaranteed confidentiality for patients
- involvement of local communities before using any therapy.
In early September, they examined 8 medications, devised to treat patients infected by Ebola and 2 vaccines aimed at prevention. These vaccines are currently being developed without following the usual authorisation process, which would take about ten years.
Although these medications have produced promising results in the laboratory, nothing guarantees that they will work, or that they will not have potentially dangerous side effects. For the time being, they are not widely available.
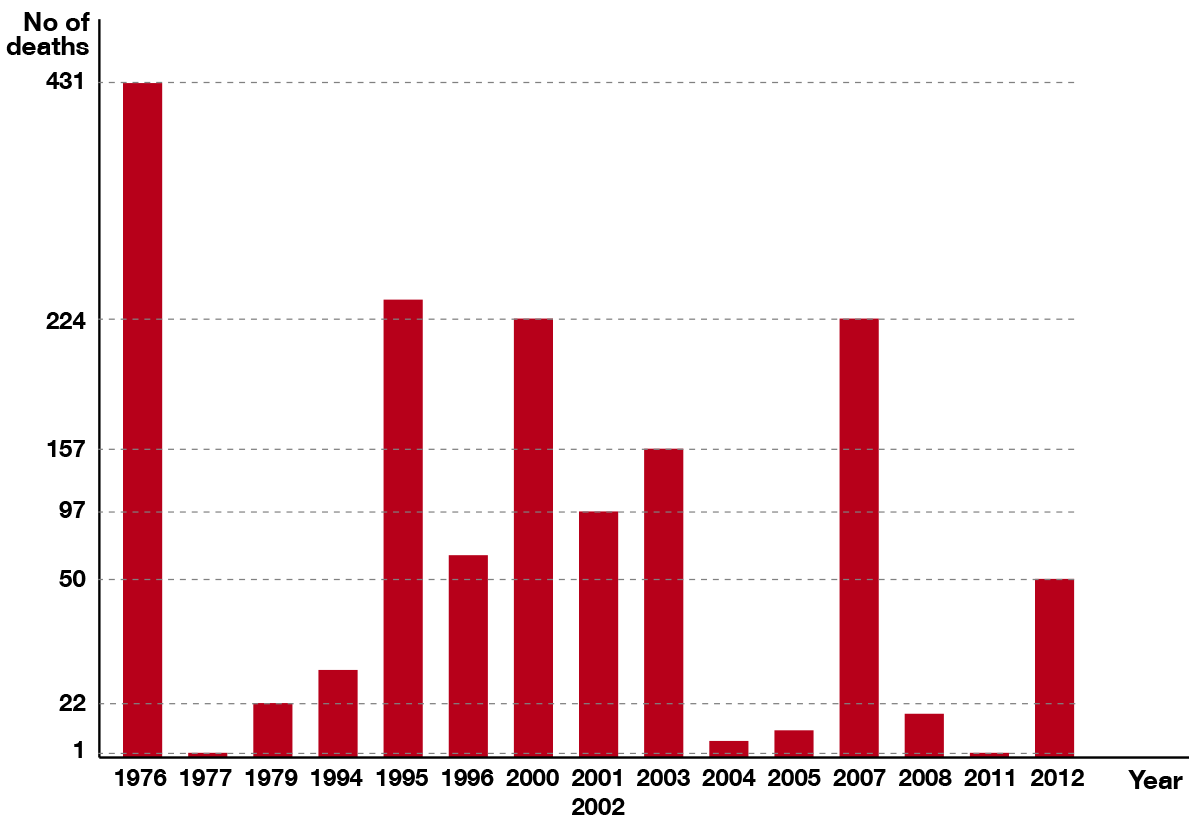
6. Is the 2014 epidemic the most serious yet?
In early September, the 2014 epidemic had already caused four times more deaths than in 1976. The first Ebola outbreaks in Sudan and Zaire resulted in 431 deaths.
The last significant epidemic was in 2007. It affected Uganda in the Gulu region, and led to 224 people dying.
PREVIOUS EBOLA EPIDEMICS :
The current epidemic is developing simultaneously, involving several outbreaks that are often far from each other, in different countries and in urban zones. However, the virus strain which was active in DRC between the end of August and mid-November, is different from the strain in Guinea, meaning that this new outbreak was not a transfer of the Guinean epidemic.
<
7. What are the strategies to fight Ebola?
The World Health Organization has declared Ebola virus disease an international public health emergency and adopted a global-scale action strategy.
Countries affected by at least one transmission
- Countries must declare a state of emergency and mobilise every possible means in their healthcare systems.
- They must also inform the population through, for example, village chiefs or religious representatives. The aim is to underline the basic safety principles.
Countries with one suspected or confirmed case or sharing borders with an affected country
- These countries must ensure close border surveillance and verify the temperature of all travellers transiting through international airports, ports and the main border checkpoints. In case of fever, the risk of Ebola must be assessed and the suspected person must be forbidden to travel.
- If the test for Ebola virus disease is positive, every possible confinement measure must be taken to prevent transmission, particularly medical surveillance of anyone who has been in contact with the sufferer.
Given the urgency of the situation, the whole international community is also actively working to combat this outbreak of Ebola and offer aid to the countries affected (health care, mobile laboratories, research). On 18 September 2014, they
adopted a unanimous resolution.
This resolution calls on all member states to provide emergency aid, i.e. field hospitals, medical teams. It also calls for an end to the isolation of Liberia, Guinea and Sierra Leone. This is the first time that the Council has described a health emergency as a
" threat to international peace and security ".
<
Useful links
Top